Pacemakers
Types, usage, precautions
There are many arrhythmic conditions that might require the implantation of a cardiac implantable electronic device (CIED). But CIEDs (i.e. permanent pacemaker or implantable defibrillator) may become contaminated during the surgical procedure before implantation. TauroPace™ is designed to prevent such complications: The solution contains taurolidine, a strong antimicrobially active molecule with antibiofilm efficacy. Taurolidine is active against a wide variety of pathogens.
Types of pacemakers explained
Which kind of CIED (i.e. pacemaker or implantable cardioverter defibrillator) is right for a patient always depends on their symptoms and diagnosis. Today, there are three devices commonly used to treat patients with advanced arrhythmic conditions:
single-chamber CIEDs with one lead connecting the pulse generator to one chamber of the heart
dual-chamber CIEDs with two leads connected to both chambers on the heart’s right side (right atrium, i.e. upper chamber, and right ventricle, i.e. lower chamber)
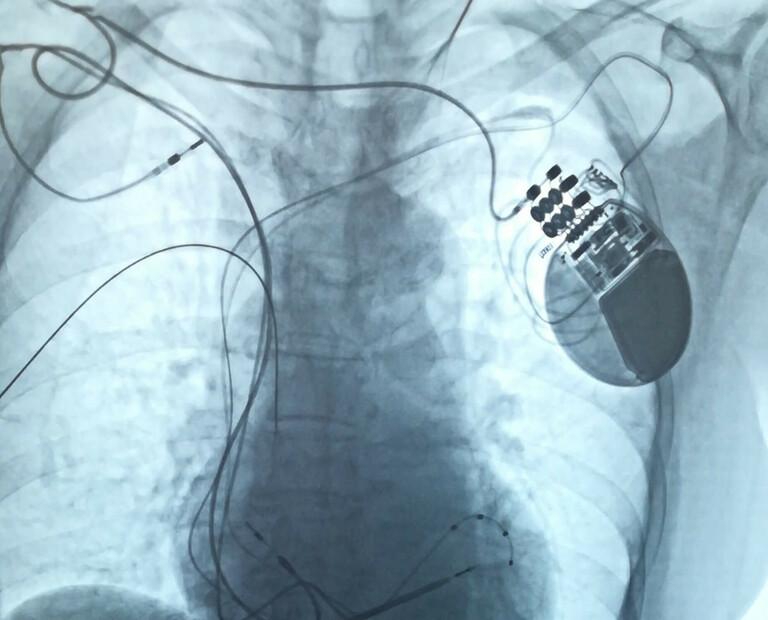
biventricular CIEDs (also known as cardiac resynchronisation therapy (CRT) devices) with three leads connected to the right atrium and both ventricles (i.e. both lower heart chambers)
TauroPace™ is designed to prevent the contamination of CIEDs.
How to use TauroPace™
TauroPace™ must be applied at several points during the surgical procedure (i.e. placing a pacemaker or defibrillator or accessing the CIED for any kind of revision procedure). The procedure can take place on an outpatient basis or during hospitalisation. Procedures may vary, depending on the patient’s condition and the physician's practices. Usually, they do not take longer than two hours.
- Patients need to remove any jewelry or other objects that may interfere with the procedure. They will also be asked to empty their bladder beforehand.
- Medical staff will place a venous access device (VAD) to inject medication or fluids (if needed).
- After the patient has lied down on the operating table, an electrocardiogram (ECG) monitor that records the heart’s electrical activity will be connected to their body with adhesive stickers. Vital signs (i.e. heart rate, blood pressure, breathing rate, oxygenation level) may also be monitored during the procedure.
- Medical staff will subsequently place large electrode pads on the patient’s chest and apply safety restraints to their torso, arms, and legs (after asking for consent).
- Some procedures may require a specific type of local anaesthesia before the procedure (so-called fascial plane blocks), which will be explained by the physician. These blocks help to minimize pain sensations and enhance recovery from the surgical procedure.
- Patients may receive a calming medication to help them relax, although they will likely remain awake during the procedure (conscious sedation).
- Medical staff will clean the skin in the area where the pacemaker will be inserted with skin disinfectants, leaving enough time for the skin to dry out completely before the incision.
- Patients will be covered with sterile adhesive drape. The surgical site might additionally be covered by an incision foil.
- Medical staff will then proceed to inject an anaesthetically active liquid directly under the skin, at the spot they plan to incise for CIED placement.
- Once the anaesthetic has taken effect, the attending physician makes a small incision beneath the left collarbone.
- The sheath (a plastic tube, including something called “introducer”) is inserted into a blood vessel at the incision.
- The lead (one, two, or three, depending on the type of pacemaker or defibrillator) will then be inserted into the blood vessel through the sheath and advanced into the heart.
- After placement, the lead(s) are wiped down with TauroPace™.
- Once the lead(s) has (or have) been placed inside the heart, the surgeon will conduct a testing to verify the proper location and functionality.
- The pacemaker generator is unwrapped and wiped down with gauze/swab soaked in TauroPace™.
- The pacemaker generator will be slipped under the skin through the incision after the lead has been connected to the generator.
- Prior to final placement, all the hardware and suture are treated with TauroPace™. The wound is subsequently closed.
- Medical staff will conduct a CIED interrogation to program the device.
- Remaining stains are cleansed with gauze/swabs soaked in skin disinfectant (not TauroPace™).
- Lastly, a sterile pressure bandage will be applied.
- A medical professional will now carry out a CIED system interrogation to verify that the system is functioning correctly.
- If the procedure takes place on an outpatient basis, patients might leave a couple of hours after the procedure.
- In general, patients should be able to resume their daily routines within a few days.
- Patients should not take a full body bath or shower in the area of the incision within two weeks following the procedure.
- Patients are also urged to refrain from lifting or pulling anything heavy for six weeks. They may be advised to not lift their arms above the head for that same period.


Living with a CIED: Dos & don’ts
Electromagnetic fields can interfere with a pacemaker's ability to sense an abnormal rhythm. Keeping this in mind, here’s what you should consider as a patient or caregiver:
Avoid devices or areas with strong electric or magnetic fields – e.g. magnetic resonance imaging.
Microwave ovens, computers, VCRs, small electrical tools, and garage door openers are safe to use.
Make sure to keep cellphones, MP3 players, and headphones at least six inches away from your pacemaker. Hold your phone on the ear opposite of your pacemaker and do not put your phone or headphones in a pocket directly above the pacemaker.
When travelling via plane, inform security staff at the airport about your condition and ask for a hand search instead of walking through the metal detector. The pacemaker will not be harmed by the metal detector, but it might trigger a false alarm. Keep the scanning process with a hand-held metal detector as short as possible.
Inform your healthcare provider about your condition before they perform any test or procedure using medical or electronic devices.
If you plan to undergo dental procedures or any type of surgery involving electrocautery, ask your attending dentist or physician to contact either the device’s manufacturer or the surgeon who has implanted it. The pacemaker might misinterpret the electrocautery as heartbeats and consequently withhold pacing.
Normal electric teeth cleaning devices are safe to use and require no special instructions.
Due to the potential magnetic interference, you cannot have an MRI (unless stated otherwise by the device’s manufacturer).